MEDICINE POSTING EXPERIENCE
Myself vaishnavi, intern welcome to my medicine blog journey where am gonna share my experience in medicine department
NOTE: THIS IS AN ONLINE E LOGBOOK TO DISCUSS OUR PATIENT'S DE-IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS/HER GUARDIAN'S SIGNED INFORMED CONSENT. HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH A SERIES OF INPUTS FROM THE AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS INTENDING TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE-BASED INPUT.
When am in third semester i used think what is medicine?NTG so special only thing we do is ask history and prescribe medicine but when am going through posting and interaction with PGS and SRS related to case taking, examinations, interlink various symptoms and subjects, etiopathogenesis and to diagnose patient just by looking his features which add on by investigation taught that it is vast and amazing subject
Here am going to share my interesting and knowledgable cases
While i was looking patient to take history and examination i saw a 14yrs old boy with an low mood about his condition, i thought why not talk to him and support him. And the case is about
https://chvaishnavirollno28.blogspot.com/2022/11/14-yrs-male-child-with-spleenomegaly.html
Through this cases i learned about
1. OPSI (OVERWHELMIMG POST SPLENECTOMY INFECTION) where patient is prone for capsulated bacteria(h. Influenze, meningococcal, pneumonnococcal-most common) as spleen is major organ for recticuloendothilial system. For which need for vaccination scheduled as
Elective - 2weeks before splenectomy
Emergency - vaccine is given an post operative day 1 or 2. If vaccine is given after surgery, antibody tirer are less
2.Post splenectomy complications?
Early:
• Haemorrhage
Injury to stomach, splenic flexure, pancreas
Delayed:
Fistula from stomach, pancreas
Subdiaphragmatic collection
Left basal atelectasis and pleural effusion
Thrombocytosis- thrombotic complications
• OPSI- H influenzae, Meningococcus
-Hematological changes
Transient - increase in RBC, increase in WBC (confused with infection) increase in platelets in first 2weeks of splenectomy
Permanent changes -
Howel jolly bodies, basophilic stippling, hyperpigmented WBC, reticulocyte in peripheral smear, these are persist life long in splenectomised patient
3.Splenomegaly causing pancytopenia as it is reticuloendothial system.
-Differential diagnosis for pancytopenia
Pancytopenia refer to reduction of all threee cells of blood i. E RBC, WBC, PLATLETS.
CAUSES OF PANCYTOPENIA
vitamin b12, iron and folic acid deficiency
Hypersplenism, aplastic anemia, leukemias, bone marrow infiltration by carcinoma, lymphoma, multiple myeloma, overwhelming infection
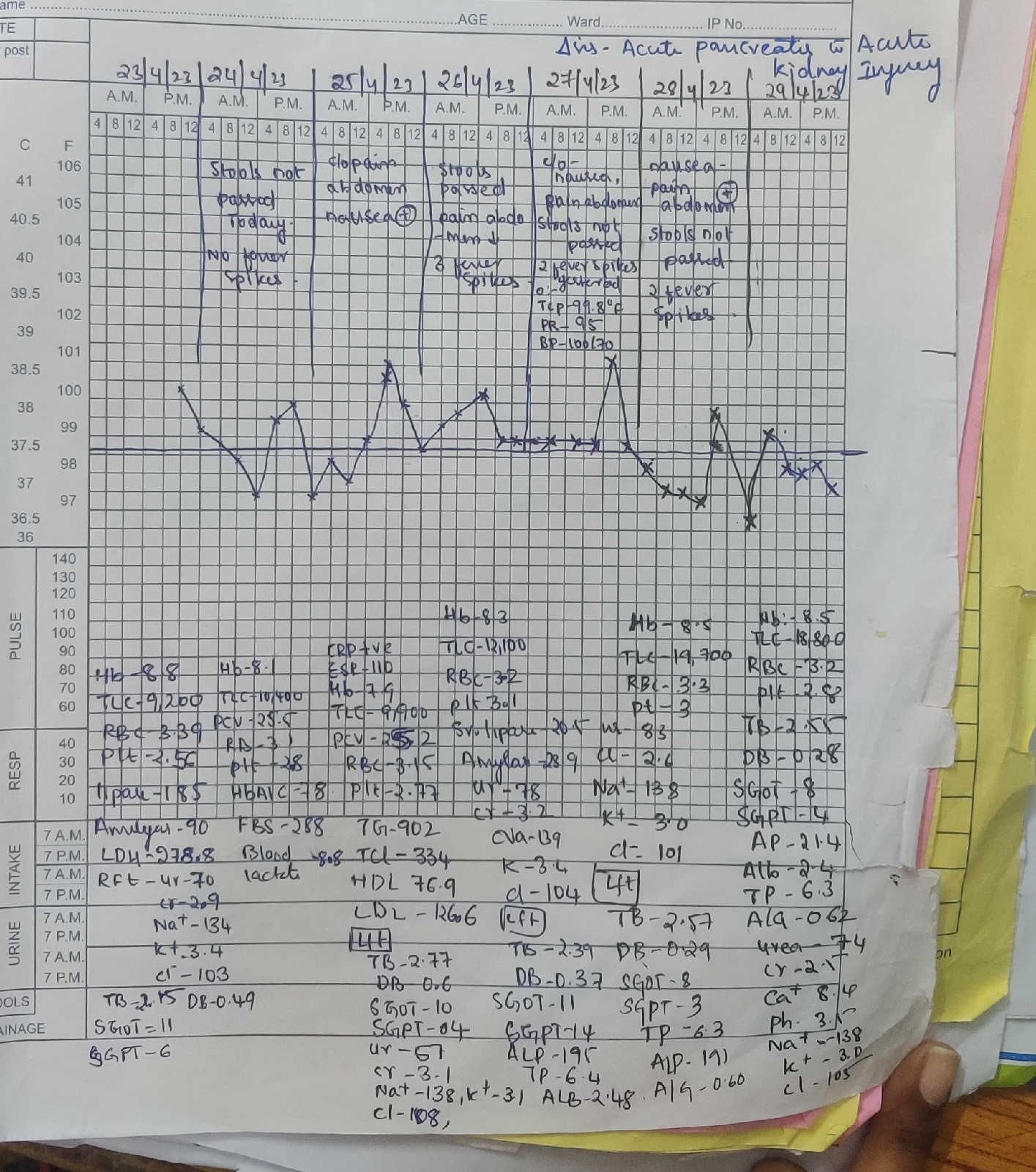
And another case i seen is Clinically distress 40yrs old female
https://chvaishnavirollno28.blogspot.com/2023/05/a-40-year-old-women-with-chest-pain.html?m=1
Learning points-
1.How triglycerides cause abdominal pain and acute pancreatic?
High level triglycerides with associated comorbidities like diabetes is major cause for acute pancreatitis after alchol and gall stones. It induces inflammatory process which leads to acute pancreatitis
2.different types of DIABETES? What is LADA?
LADA is characterized by adult-onset diabetes and circulating autoimmune antibodies; thus, patients may present clinically with characteristics of both type 1 and type 2 diabetes (2–5). Typically, the clinical features of type 1 diabetes seen in LADA include a lower BMI compared to what is typical in type 2 diabetes and autoimmunity against one or more of the following antibodies: islet cell autoantibodies (ICA), autoantibodies to glutamic acid decarboxylase (GAD), tyrosine phosphatase–related islet antigen 2 (IA-2), and insulin autoantibodies (IAA) (4,5). The characteristics of type 2 diabetes that may present in LADA include older age at onset and insulin resistance or deficiency. Characteristics of LADA tend to include an intermediate level of β-cell dysfunction between those in type 1 and type 2 diabetes, faster decline of C-peptide compared to type 2 diabetes, and a level of insulin resistance that is comparable to type 1 diabetes (4). β-Cell decline is variable in LADA, as measured by C-peptide levels
Another case of patient with fever associated with multiple ulcers all over the body
https://chvaishnavirollno28.blogspot.com/2023/01/35-year-old-female-with-fever-and.html
Learning points
1.How methotrexate toxicity leads to pancytopenia?
2.Methotrexate cause folic acid deficiency
3.methotrexate toxicity treatment?
Stop taking methotrexate and give iv infusion with leucovorin glucardipase with folic acid supplemention.
4.features of methotrexate toxicity?


Comments
Post a Comment