Ckd case
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient' problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
57yr old male patient farmer by occupation presented with cheif complaints of
Bilateral lower limbs swelling associated with pain since 5 days
Decrease urine output since 5 days
Fever during dialysis since 2 days.
HOPI:
Patient was apparently alright 1 year back following which he developed bilateral lower limb swelling associated with shortness of breath, pain in flank and decreased urine output and fever then he visited local physcian where he was diagnosed with chronic renal failure and referred to nephrologist near by and started medical management for CKD.
Since then patient is on conservative management for CKD for 6 months.
6 months back he developed sudden onset of shortnessof breath associated with generalised body swelling then he went to a nephrologist near by and hemodialysis was initiated through RT IJV. 10 sessions of hemodialysis was done and Patient was referred to NIMS for further evaluation.
Patient was hemodynamically stable when he consulted to nephrologist in NIMS and they advised to pause the dialysis and managed with medication for 1 month and removed central line.
As patient felt better and re-energise patient didn't follow up at NIMS for 4 months and started doing his routine farming.
2 months back patient developed similar episodes of SOB at rest and pedal edema and undergone dialysis at Osmania through permacath placed in Rt IJV.
Since then patient is on maintainance Hemodialysis.
Since 2 days patient having chills and fever during dialysis and hypotension.

Personal history :
Appetite : decreased
Diet : mixed
Sleep : adequate
Bladder : decreased urine output
Bowel movements: regular
Addictions :absent
General examination:
Pallor: absent
Icterus: absent
Cyanosis : absent
Clubbing : absent
Lymphadenopathy : absent
Edema : present B/L pitting type of pedal edema


Vitals:
Temperature: afebrile
Pulse: 119 bpm
Blood pressure:140/80 mm of hg
Respiratory rate : 28 bpm
SpO2 : 96 on RA
GRBS : 358 MG/DL
Systemic examination:
Cardiovascular system
S1, S2 - heart sounds heard
Pericardial rub - absent
Jvp is raised
ECG:


Respiratory system:
Patient examined in sitting position
Inspection:-
oral cavity- Normal ,nose- normal ,pharynx-normal
Chest shape : Barrel
Trachea is central in position.
Palpation:-
All inspiratory findings are confirmed
Trachea central in position
Apical impulse in left 5th ICS,
Chest movements bilaterally symmetrical
AUSCULTATION
Decreased air entry on Rt side
B/L crepts present ( Rt >lt)

Abdomen examination:
INSPECTION
Shape : distended
Umbilicus:normal
Movements :normal
Visible pulsations :absent
Skin or surface of the abdomen : normal
PERCUSSION- tympanic
AUSCULTATION :bowel sounds heard
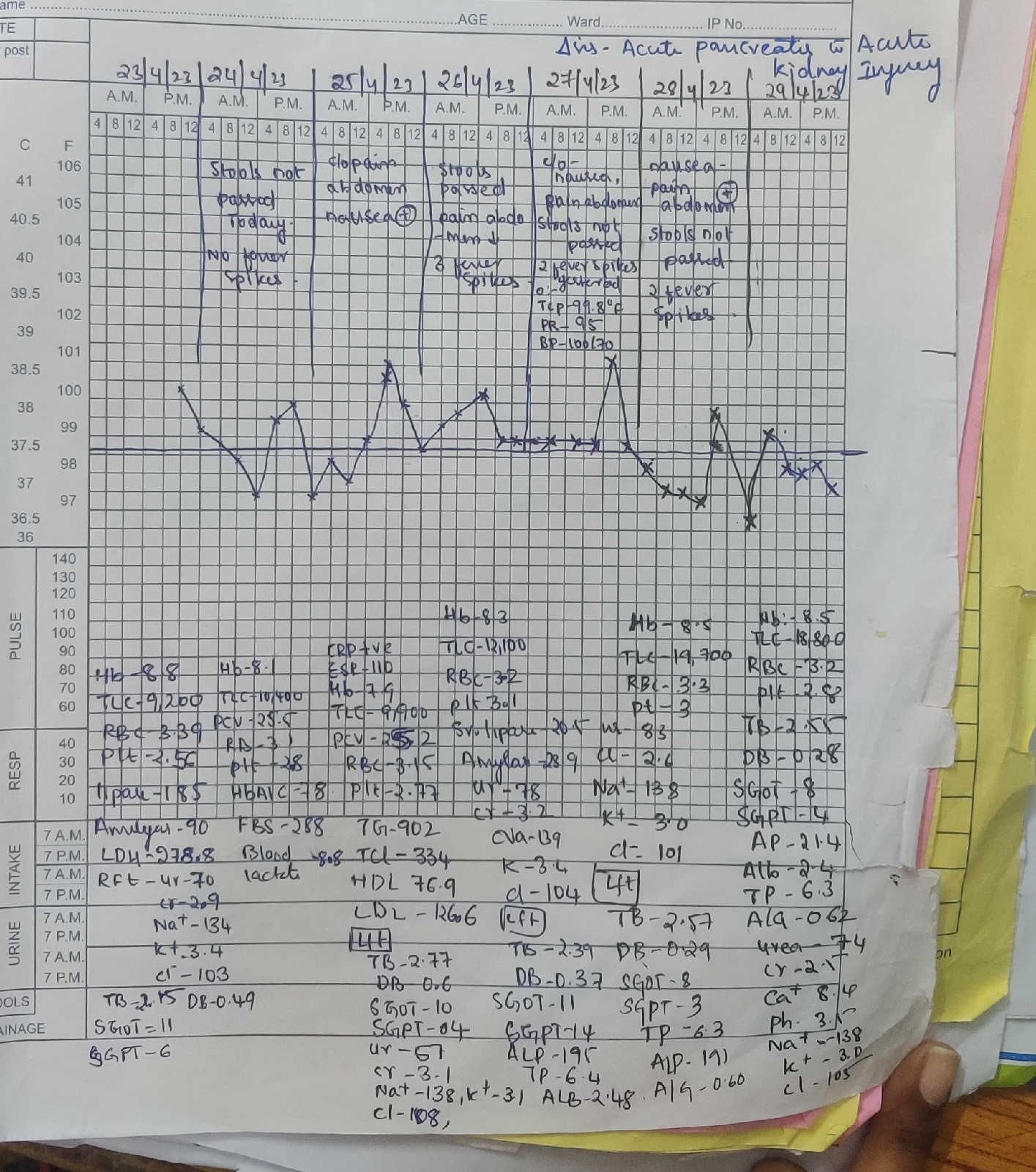
USG :

LABS:

FEVER CHART:

PROVISIONAL DIAGNOSIS:
CKD ON MHD(hepatic hemosiderosis in maintenance hemodialysis)
Treatment:
Iv paracetamol
28/06/22
On dialysis
Patient was stable and treatment is given
29/06/22
Bp 110/80
Under treatment
Fever reduced
29/06/22
Patient was discharged

Comments
Post a Comment