39 YEAR OLD MAN WITH ALTERED SENSORIUM WITH KIDNEY DISEASE
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 39 Yr old male , electrician by occupation, resident of nalgonda,came to causality on 09/11/21 with..
CHEIF COMPLAINT:
Fever(10days back), loss of appetite(2days back) ,Involuntary movement of upper limbs and drowsiness(1day back)
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 10 days back then he developed low grade fever with chills intermittently and nausea.And he also had cough but no discharge.
-Loss of appetite since 2 days .
Since one day ,pt was unable to speak. but understanding commands .
Since yesterday morning(8/11/21) , patient was having 2 episodes of involuntary movements of b/l upper limbs and was drowsy since morning .
Left leg has slight swelling from the date of admission and it is progressive
No h/o of headache, blurring of vision, vomiting.
No h/o loose stool.
All his medical history started 8 month's ago
8 months ago with the c/o low back ache , pain abdomen went nalgonda hospital,where incidently detected with creatinine level 5mg/dl.and diagnosed as RENAL CALICULI WITH INCREASED SERUM CREATININE .
His urine output was good and he had no pedal edema or sob. He was told to have renal failure and was on medication since then.
He even had h/o wt loss and loss of appetite and low grade fever.
He was having intermittent back pain since then .
After 2 months in August ,
** August last week , 2021 -- c/o left lower limb weakness, slow gradually progressed to right LL -- B/L Paraplegia i .e flaccid paraplegic- MRI was done --and they diagnosed as POTTS SPINE
Used ATT for 15 days and stopped , due to nausea and loss of appetite, patient was bedridden since, then and used unani medication.
Pt was neglected and using Unnani medications inspite of advising to use ATT.
**H.D was adviced 2 months ago - but didn't get it done due to fear of death ( among relatives deaths on H.D+)
** Since September 2021--Bed sores developed, 1 daily dressing done ,but patient was active and talks to everyone.

N/o h/o DM , HTN, EPILEPSY, ASTHMA.
PERSONAL HISTORY:
** He has normal appetite , consumes mixed diet with regular bowel movements, he was on Foley's since 6 months .
Sleep-adequate
No addictions
FAMILY HISTORY: his sister and uncle had kidney disease.
O/E :-
Pallor+
No icterus, cyanosis, clubbing edema , lymphadenopathy.
Pedal edema on left leg which pitting type.
VITALS ON ADMISSION:-
Temp:- 101F
PR:- 92 BPM
RR:-14 cpm
BP: 90/60 MMHG
Spo2:- 83 % at RA
GRBS:- 195 MG%
CVS:- S1 S2+ ,NO MURMUR
RS:- BAE+ , NVBS+
P/A SOFT ,NT
CNS:- Eye opening to pain
No verbal response
No meningeal signs(brudzinski sign and kernig's sign both are negative)
GCS:- E2 V1 M5. 8/15
PUPILS--B/L mid dilated unequal(Rt>Lft)
Plantars-- B/l Flexion
Power- --. RT. LT
Upper limb - 5/5. 5/5
Lower limb- plegia plegia(0/5)
Tone --
Upper limb- Increased.Increase
Lower limb- Decreased.decreased.
Reflexes:- RT. LFT
B- absent. 2+
T-. 3+. 3+
S-. 2+. 2+
K-. Absent. Absent
A-. Absent. Absent.
Provisional diagnosis:-
1) ALTERED SENSORIUM
2)SECONDARY TO? POST ICTAL CONFUSION WITH ? ACUTE ISCHEMIC CVA( PARIETO TEMPORAL AREA) . or ? uremic encephalalopathy.
3) ? TB - VASCULITIS/ SEPTIC INFARCT
4) PARAPLEGIA SECONDARY TO POTTS SPINE
5) CKD
6) ANEMIA
7) GRADE 3 BED SORE.
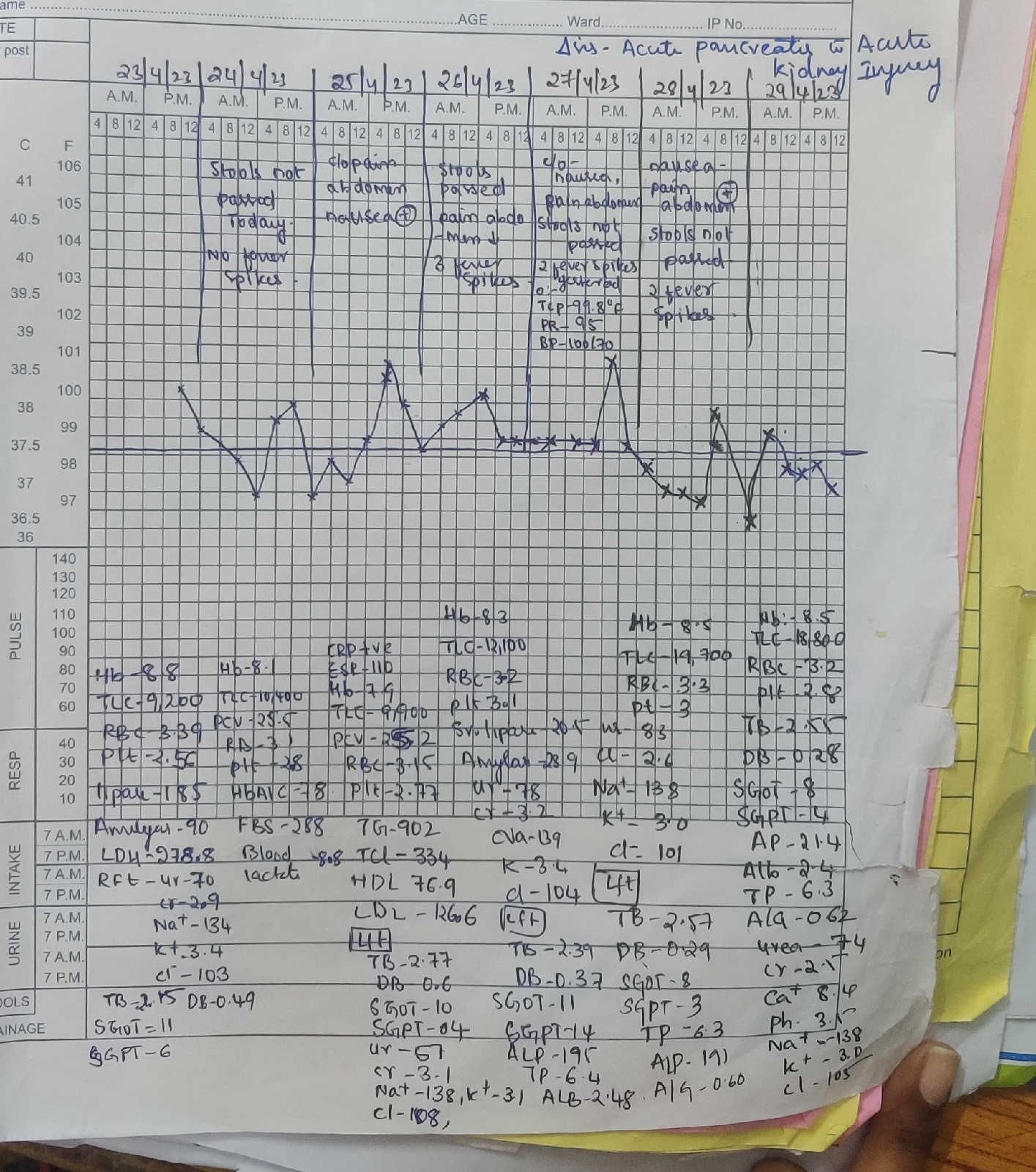
Investigations:-
HB:- 3.8
PLT :- 61000
BGT:- A Positive
Na-137
K-4.3
Cl-98
Sr.creat-4.2
LFT:-
TB- 0.92
DB-0.27
SGOT-18
SGPT-24
ALP-375
TP- 4.7
ALBUMIN:-2.0
A/G :-0.76
LDH:- 225
Blood urea- 247
Rbs-143
Serology--NEGATIVE
C-reactive protein-- POSITIVE-2.4 mg/dl.
TREATMENT :-
1) IVF NS-2 units
RL-1 unit
Dns- 1 unit @ 100 ml/hr
2) Inj. Optineuron 1 amp in 100 ml NS IV OD
3) Inj. Levipil 1 gm IV stat--500 mg iv bd
4) RT Feeds milk + Protein powder 4th hourly..free water 200 ml 4th hourly
D1-5) Inj. Ceftriaxone 2gm iv bd
6) Inj. Neomol 1 gm IV SOS
7) Tab. Dolo 650 mg RT TID
8) Inj. Pantop 40 mg IV OD
9) ATT According to renal clearance and wt.
10) GRBS 12 TH HOURLY
I/O CHARTING
BO/PR MONITORING.
11) INJ. Pan 40 mg /Iv /Od
12) Inj. ZOFER 4 mg iv bd.
12/11/21
They suspect the DVT ON LEFT LEG BECAUSE IT HAS SWOLLEN.
13/11/21
He get dialaysed after that he had better senoruim .
18/11/21
Patient had increased requirements of inotropes to maintain since 6pm
No episode of tachypnea.
No response to verbal and painful stimuli.
19/11/21
At 6:15am patients saturation was not recorded with absent central pulses,8cycles of cpr was done as per 2020aha guidelines,but he couldn't be resuscitated.

Comments
Post a Comment